
Yen Chow and Jorge Cabrera [Updated Sept 21, 2015]
A cardiac arrest has been called on the floor and you happen to arrive before the crash cart. CPR is in progress and mask ventilation is being performed with an oral airway. A lot of suctioning is required for vomit in the airway. There is difficulty ventilating despite optimizing position, two person bag-valve-mask ventilation, additional nasal airways and maximal jaw thrust. There is limited access to the head of the bed in the patient’s room. As an airway clinician on the code blue team you carry a bougie and a cuffed 6.0 endotracheal tube with you.  Intubation and extraglottic airway equipment still has not arrived. Pulling out your bougie and tube, you take out the patient’s dentures and use the oral airway as a bite block. You find the epiglottis with your middle and index fingers inserted into the mouth and guide the bougie into the glottic opening feeling tracheal ticks and hold-up to confirm. The tube slides over the bougie. Successful ventilation occurs without chest compressions missing a beat and the code continues.
Intubation and extraglottic airway equipment still has not arrived. Pulling out your bougie and tube, you take out the patient’s dentures and use the oral airway as a bite block. You find the epiglottis with your middle and index fingers inserted into the mouth and guide the bougie into the glottic opening feeling tracheal ticks and hold-up to confirm. The tube slides over the bougie. Successful ventilation occurs without chest compressions missing a beat and the code continues.
Blind digital intubation using one’s fingers to locate the laryngeal inlet and then guide an endotracheal tube into the trachea is not a commonly used skill nor is it talked about much. Some clinicians have trained and practiced it and there have been anecdotal cases where it has been successful in difficult airways where direct laryngoscopy has failed, usually from too much fluid soiling the airway.
This technique is best facilitated with a bougie to guide the tube delivery. The advantage of the bougie is that the smaller diameter allows it to be easily manipulated into small spaces and it is easier to pass into the trachea. One’s finger may also be able to feel it guided into the trachea provided the finger is long enough to reach a given patient’s mouth opening and air way anatomy. Bougie tracheal ticks and hold-up can give added confirmation if one is uncertain of delivery into the
way anatomy. Bougie tracheal ticks and hold-up can give added confirmation if one is uncertain of delivery into the
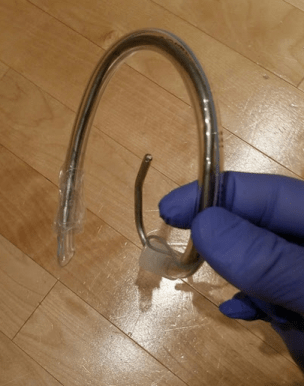
trachea. A precurved bougie can help (either keeping the straight bougie curled in a plastic bag or else using the Introes Pocket Bougie).
The usual maneuvers to railroad a tube over a bougie will be helpful including left turn at the laryngeal inlet and pulling tongue and jaw forward. Smaller tubes and shrouded tip tubes will railroad easier.
The steps are
- Stand on the left side of the
patient, remove dentures - Insert middle and index fingers of left hand in patient’s mouth
- Use left hand middle finger to follow the curve of
tongue posteriorly to feel the epiglottis edge
- Lift up epiglottis with your middle finger
- Insert the bougie down lateral side of middle finger between middle finger and index finger
- Use the index finger to put guide bougie into the larynx

James M Rich describes a case of successful blind digital intubation with a bougie introducer [1].
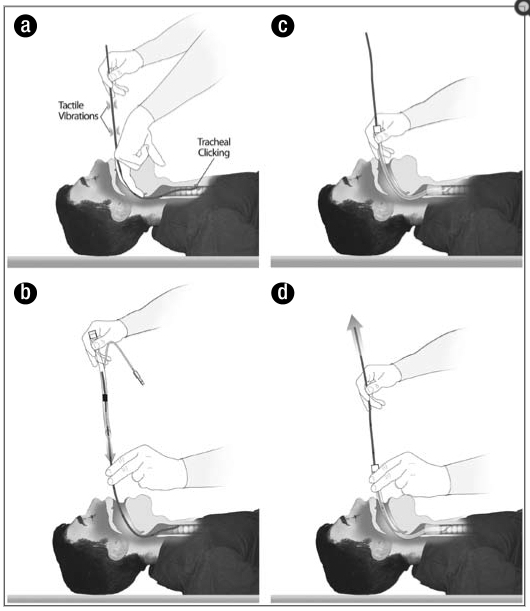
“Bougie-assisted digital intubation.
(a) After the epiglottis is identified by palpating it with the long finger of the left hand, the bougie is threaded through the glottis and advanced into the trachea. Tracheal clicking elicits tactile vibrations, which confirm tracheal placement of the bougie.
(b) The bougie is withdrawn slightly so that the 25-cm mark is at the corner of the lip. The endotracheal tube is threaded over the bougie while the bougie is stabilized in place.
(c) With the bougie held in place, the endotracheal tube is turned a quarter turn to the left and then advanced to an appropriate depth.
(d) The tube is held in place while the bougie is withdrawn. Tracheal intubation is then confirmed using capnography or an esophageal detector device.” [1]
“Standing at the side of the patient (face to face), the left index and long fingers were inserted into his mouth and along the tongue to a depth that made it possible to digitally identify the epiglottis, the rima glottis, and posterior cartilages. With the fingers pressing the epiglottis against the pharyngeal wall, a bougie was passed along the axis of the long finger (stabilizing it between the index and long finger) and inserted through the glottis, where it elicited tracheal clicking, and was then advanced to a depth of 25 cm from the corner of the lip. The endotracheal tube was then passed over the bougie into the trachea, which was confirmed by capnography. The digital intubation required less than 1 minute.” [1]
Other alternatives are to guide either the endotracheal tube alone or stylet-shaped to curve around the tongue.
 [Ref 3]
[Ref 3]
 [Ref 4]
[Ref 4] [Ref 5]
[Ref 5]
Circumstances that blind digital intubation will be helpful:
- Impossible visualization with fluids blocking direct or indirect views including massive hematemesis, hemoptysis, airway bleeding, and regurgitation from bowel obstruction or full stomach.
- Direct view not possible due to inability to access the head of patient or inability to manipulate head and neck into “sniffing/ear-to-sternal-notch” position.
- Lack of functional airway equipment (including suction, laryngoscope, rescue airways like extraglottic devices)
- Finger, bougie, tube available
Dependent on
- Intubator factors: size of hands/fingers, length of fingers;
- Patient factors: airway anatomy allows one’s fingers to reach the laryngeal inlet. Smaller sized patients (pediatric?) likely working better as long as the fingers can fit into the oropharynx (one may need to use smaller fingers like the little finger). Airway distortion and foreign bodies may make it more difficult to recognize anatomy by touch.
- Requires adequate mouth opening; no teeth is easier, if dentures are present, take them out
- Requires patient not to bite you: must be unresponsive, consider double gloves or using a bite block
- Familiarity … a lost art that is not practiced nor taught much
If blind digital intubation is well trained it can occur rapidly within 20 seconds and requires no particular positioning. If considered for rescue airway/ventilation (an unstable desaturating patient) one must choose which airway intervention is fastest and most reliable to restore ventilation and oxygenation. Familiarity and practice with this technique may make it a viable choice however supraglottic airways in general are the fastest and most reliable choice where optimal BVM fails. Well trained scalpel finger bougie cricothyrotomy can also be very rapid and very reliable within 20 seconds. Blind digital intubation however can potentially have a place to rescue a failed airway as well.
Thanks to Thomas Dolven, Minh Le Cong, George Kovacs, Rich Levitan and the rest of #FOAMed for ideas and inspiration!
Other links and references
Life In The Fast Lane and SOCMOB Blog have some great summaries on blind digital intubation with references.
- Rich JM. Successful blind digital intubation with a bougie introducer in a patient with an unexpected difficult airway. Proc (Bayl Univ Med Cent). 2008 Oct; 21(4): 397–399.
- Benumof J, Hagberg CA. Benumof’s Airway Management: Principles and Practice 2nd ed. 393-398
- Nancy Caroline’s Emergency Care in the Streets 7th ed. 435-437
- Gad Estis YouTube. Digital Intubation. https://www.youtube.com/watch?v=-vZniHPPyYg
- emsce1 YouTube. Digital Intubation. https://www.youtube.com/watch?v=WbQEJ52Qa-w

Pingback: Tactile Bougie (Blind Digital) Intubation | Prehospital and Retrieval Medicine - THE PHARM dedicated to the memory of Dr John Hinds
Pingback: Global Intensive Care | You want me to stick my finger where?