
Should you GOOSE the tube, don’t lose it, USE it!
(Updated 2015-10-04 Yen Chow)
You have a patient with decreased level of consciousness from a closed head injury. They are not protecting their airway and present with active vomiting and gurgling sounds in their airway. You try your best with c-spine precautions and try to position the patient’s head and neck to keep the spine immobilized in alignment (perhaps turned on a backboard). You know that you have to intubate this patient as they are not maintaining their airway and are at high risk of aspiration. Gastric regurgitation continues despite continuous suctioning.
Having extra suctions are always good in this situation to clear the fluids adequately and also as backup in case one suction gets plugged up by particulate matter/fails. If the yankauer plugs up too much consider taking the suction tubing off and sinking the end of it into the airway to suction out the bits.
Here is a tip on using the tubing for high volume suction.
https://twitter.com/TBayEDguy/status/556237489510166528
Large diameter rigid suction sticks/scoops can help and are commercially available.

What do you do if your powered suction breaks?
‘https://twitter.com/TBayEDguy/status/650310791107735552
‘https://twitter.com/TBayEDguy/status/650312476303618048
‘https://twitter.com/TBayEDguy/status/650313725598023680
‘https://twitter.com/TBayEDguy/status/650314812367376386
If you have practiced intubations with patients rolled onto their side, you can certainly try to see if you can secure the airway this way however it is not the optimal position. You could consider doing laryngoscopy mainly to help airway clearance and see if you can intubate. I still count this as an intubation attempt even if all you do is use suction.
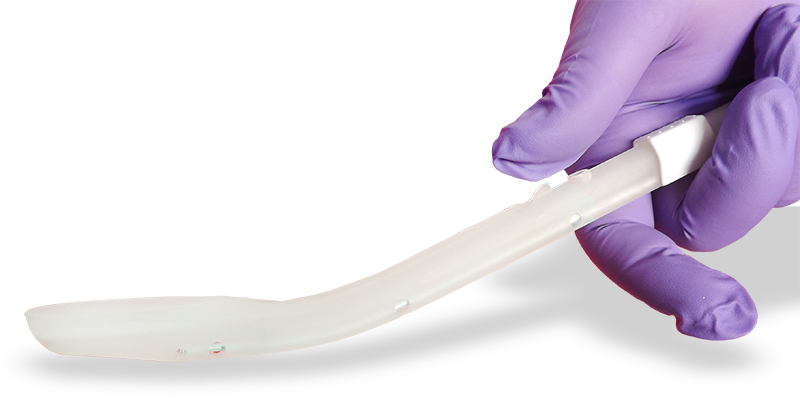
If you can’t intubate, consider goosing the tube for esophageal diversion and then moving to a better position for optimized look laryngoscopy.

Pingback: Overwhelming regurgitation/hematemesis – Diverting Esophageal Tube | Prehospital and Retrieval Medicine - THE PHARM dedicated to the memory of Dr John Hinds
VL..is not always equal. Those with channels like Pentax 200..king vision…vividtrac..or AirTraq..with the new monitor adapter..allows you to maneuver in tighter space. You may leave the suction apparatus on the right. Standard geometric VL blades need more room to allow passage of the styled..endotracheal tube as taught by Jim Ducanto.
LikeLike
Thanks for the thoughts in this Jose. Limited mouth opening and limited upper airway space are always a challenge! I am not sure if channeled vs unchanneled will make the difference in all situations. Each device’s unique blade angle, handle size, blade shape and cross sectional area etc can make or break it in terms of being able to get it positioned into the mouth. Some patient anatomy or pathology may lend itself well to any one type of IL/DL and less so to a different IL/DL. Unchanneled blades can always have a blade-shaped styletted tube or bougie passed to the target by hugging the posterior surface of the blade. I think one of the biggest factors still is the operator’s familiarity and experience in use of any particular device.
LikeLike
Question posed to the #airwayMafia: “Do channeled VL/IL’s have an advantage over standard geometry VL/IL in limited mouth opening, limited space?”
====
From George Kovacs (@kovacsgj): “Theoretically but the 3 – Airtraq, KV and AWS all have relatively large AP profiles. To insert in the large patient especially immobilized trauma pt the proximal screen portion may not allow entry (KV>AWS>AWS). Can remove KV screen and re-attach when blade is in the mouth. Rotation of device (90* CW) for entry works re chest impingement but requires even more mouth opening as lateral (side-side) profile is even larger. Other issue is ETT advancement to committed trajectory from channel. Usually manageable with several maneuvers but can an issue.”
====
Yen: “Thanks George
My thoughts are similar in experience with the Airtraq. My playing with the King Vision is very limited but I do find that it seems to be a larger blade to try to fit into the mouth and could be limiting. I do also find the long length of it to be frustrating even when the screen is taken off.
I generally find I like the freedom of unchanneled tube delivery but that may be mostly because I am more practiced at it. I generally find the channeled to be fine. Some people seem to do well with one and not the other. Comes back again to using what you are most familiar and practiced with.”
LikeLike
Sorry, no the channeled blades are only of advantage if you can get them in to the mouth, and tube delivery is not guaranteed in these cases. I have a few cases with the Pentax, I’ll dig them up. I had a few congenital abnormalities. But the GlideScope blade we had at the time was the big blade (not useful). The Pentax was really made to solve the small Japanese airway, and fails in the tall big Nordic Europeans we have here in Wisconsin (and Minnesotta). Later versions of the Pentax blade are better, including the one with a 12 mm blade extension over the original model.
Jim DuCanto, M.D.
LikeLike