What are all the things that must be done to achieve optimal BVM?
Here are some ways to remember and various pearls. Continue reading “Optimal Bag Mask Valve Ventilation”

What are all the things that must be done to achieve optimal BVM?
Here are some ways to remember and various pearls. Continue reading “Optimal Bag Mask Valve Ventilation”
Collected tweets on managing persistent flooding of the airway with fluids (blood or gastric fluids)
During a slower emerg shift on Christmas day 2015, I finally designed push dose pressor labels and sticker orders/instructions for mixing that work with the labels in our emergency department. I use these for resuscitations and teaching.
Some time ago, in this galaxy, our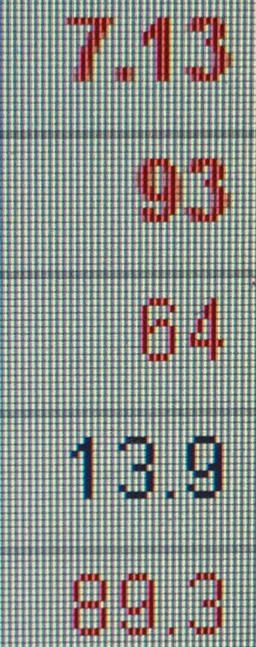 good friend Jorge Cabrera was faced with managing respiratory failure in a 55’ish year old man with BMI of 92 (ht 6 feet, wt 675 lbs (307kg). This patient was initially admitted with an upper gastrointestinal bleed with congestive heart failure and a history of obstructive sleep apnea. He had required mechanical ventilation but was weaned off recently. His recent intubation involved 2 attempts by anesthesia with the first attempt being failed Mac 3 direct laryngoscopy and the second attempt being a successful glidescope intubation.
good friend Jorge Cabrera was faced with managing respiratory failure in a 55’ish year old man with BMI of 92 (ht 6 feet, wt 675 lbs (307kg). This patient was initially admitted with an upper gastrointestinal bleed with congestive heart failure and a history of obstructive sleep apnea. He had required mechanical ventilation but was weaned off recently. His recent intubation involved 2 attempts by anesthesia with the first attempt being failed Mac 3 direct laryngoscopy and the second attempt being a successful glidescope intubation.
The patient was now in hypercapnic hypoxic respiratory failure despite all treatment including NIPPV. His arterial blood gas was not improving despite CPAP or BiPAP (EPAP of 12).
pH 7.1 PaCO2 90’s PaO2 60’s SaO2<90’s
Continue reading “Definitive airway on BMI 92 hypoxic hypercapnic respiratory failure”
Make electrical safety a top priority with this setup, please.
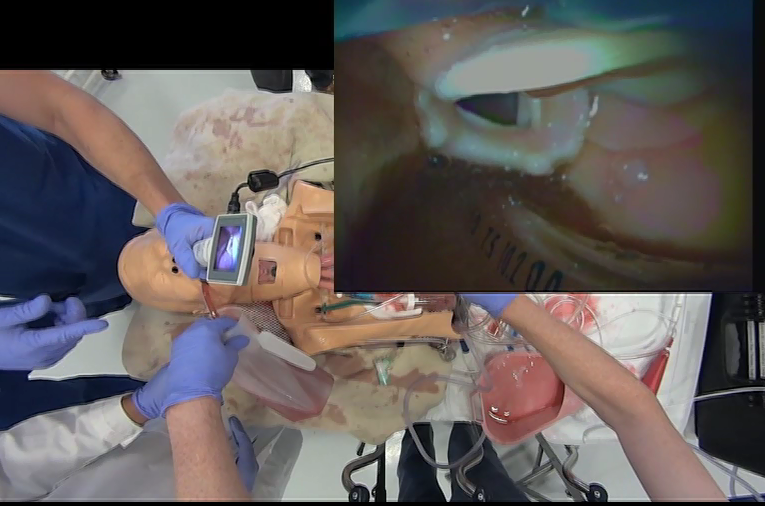
Here are the basic construction instructions to create the Suction Assisted Laryngoscopy Airway Decontamination (SALAD) simulator (AKA “VomiQuin”) from the airwayNatic @jducanto.

Should you GOOSE the tube, don’t lose it, USE it!
Continue reading “Overwhelming regurgitation/hematemesis – Diverting Esophageal Tube”
 In airway management, oxygenation and ventilation are the overriding priorities and fluids in the airway must be avoided and managed at all costs.
In airway management, oxygenation and ventilation are the overriding priorities and fluids in the airway must be avoided and managed at all costs.
It’s not about plastic in the trachea
– Rich Levitan (@airwaycam)
When indirect control of the epiglottis and laryngeal exposure proves difficult by the traditional Mac blade approach of placing the blade tip in the valleculae, consider repositioning the blade like in Miller blade technique to directly lift the epiglottis.
Continue reading “Response to difficulty: Use Mac Like Miller”
Yen Chow and Jorge Cabrera [Updated Sept 21, 2015]
A cardiac arrest has been called on the floor and you happen to arrive before the crash cart. CPR is in progress and mask ventilation is being performed with an oral airway. A lot of suctioning is required for vomit in the airway. There is difficulty ventilating despite optimizing position, two person bag-valve-mask ventilation, additional nasal airways and maximal jaw thrust. There is limited access to the head of the bed in the patient’s room. As an airway clinician on the code blue team you carry a bougie and a cuffed 6.0 endotracheal tube with you.  Intubation and extraglottic airway equipment still has not arrived. Pulling out your bougie and tube, you take out the patient’s dentures and use the oral airway as a bite block. You find the epiglottis with your middle and index fingers inserted into the mouth and guide the bougie into the glottic opening feeling tracheal ticks and hold-up to confirm. The tube slides over the bougie. Successful ventilation occurs without chest compressions missing a beat and the code continues.
Intubation and extraglottic airway equipment still has not arrived. Pulling out your bougie and tube, you take out the patient’s dentures and use the oral airway as a bite block. You find the epiglottis with your middle and index fingers inserted into the mouth and guide the bougie into the glottic opening feeling tracheal ticks and hold-up to confirm. The tube slides over the bougie. Successful ventilation occurs without chest compressions missing a beat and the code continues.
Continue reading “Bougie-Assisted Tactile Blind Digital Intubation”


{kind=link}